Free Michigan 514 Template in PDF
The Michigan 514 form serves as a crucial document for businesses navigating the complexities of tax clearance in Michigan. Specifically designed for sole proprietorships, partnerships, limited liability companies, and corporations that have sold the majority of their assets, this form facilitates the request for a Conditional Tax Clearance. It is essential for businesses that plan to maintain their corporate shell while continuing to file tax returns until a final decision is made regarding dissolution. Completing the form requires detailed information, including the name of the business, the Federal Employer Identification Number, and the owner’s social security number, among other specifics. Additionally, businesses must disclose operational details, such as whether they will continue business activities post-clearance and any outstanding tax returns. The form also includes a certification section where the owner or authorized member must affirm the accuracy of the provided information under penalty of perjury. To ensure compliance, all unfiled Michigan tax returns and associated remittances must accompany the submission of the form. Properly completing and submitting the Michigan 514 form is a vital step for businesses aiming to maintain compliance and facilitate smooth transitions during asset sales.
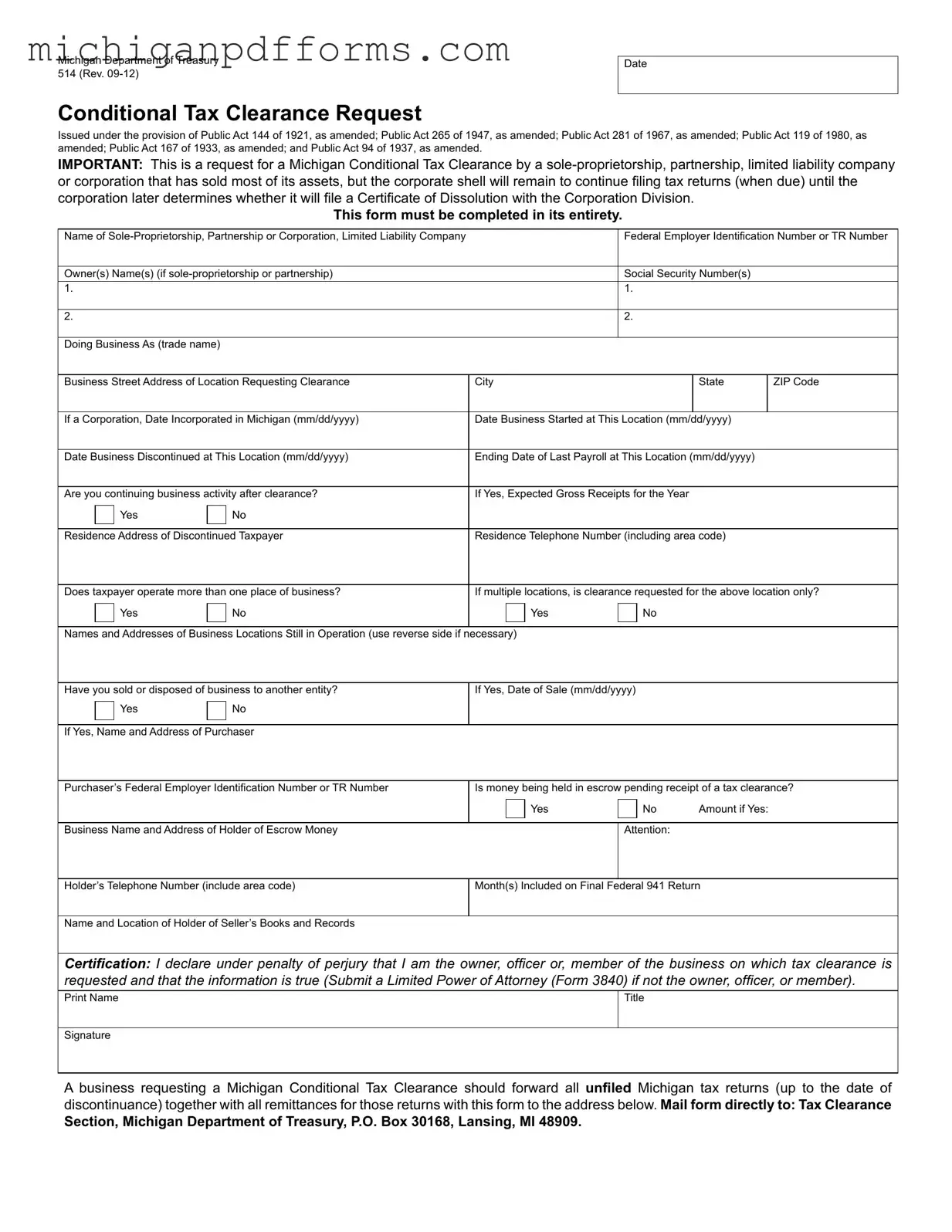
Form Example
Michigan Department of Treasury 514 (Rev.
Date
Conditional Tax Clearance Request
Issued under the provision of Public Act 144 of 1921, as amended; Public Act 265 of 1947, as amended; Public Act 281 of 1967, as amended; Public Act 119 of 1980, as amended; Public Act 167 of 1933, as amended; and Public Act 94 of 1937, as amended.
IMPORTANT: This is a request for a Michigan Conditional Tax Clearance by a
This form must be completed in its entirety.
Name of |
|
|
|
Federal Employer Identiication Number or TR Number |
||||||||
|
|
|
|
|
|
|||||||
Owner(s) Name(s) (if |
|
|
|
Social Security Number(s) |
|
|||||||
1. |
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Doing Business As (trade name) |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
Business Street Address of Location Requesting Clearance |
City |
|
|
State |
|
ZIP Code |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
If a Corporation, Date Incorporated in Michigan (mm/dd/yyyy) |
Date Business Started at This Location (mm/dd/yyyy) |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
||
Date Business Discontinued at This Location (mm/dd/yyyy) |
Ending Date of Last Payroll at This Location (mm/dd/yyyy) |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Are you continuing business activity after clearance? |
If Yes, Expected Gross Receipts for the Year |
|
|
|
||||||||
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||||||
Residence Address of Discontinued Taxpayer |
Residence Telephone Number (including area code) |
|
||||||||||
|
|
|
|
|
|
|||||||
Does taxpayer operate more than one place of business? |
If multiple locations, is clearance requested for the above location only? |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Names and Addresses of Business Locations Still in Operation (use reverse side if necessary) |
|
|
|
|
|
|||||||
|
|
|
|
|
||||||||
Have you sold or disposed of business to another entity? |
If Yes, Date of Sale (mm/dd/yyyy) |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
If Yes, Name and Address of Purchaser |
|
|
|
|
|
|
|
|
||||
|
|
|||||||||||
Purchaser’s Federal Employer Identiication Number or TR Number |
Is money being held in escrow pending receipt of a tax clearance? |
|||||||||||
|
|
|
|
|
|
|
Yes |
|
No |
Amount if Yes: |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|||||
Business Name and Address of Holder of Escrow Money |
|
|
|
Attention: |
|
|
|
|||||
|
|
|
|
|||||||||
Holder’s Telephone Number (include area code) |
Month(s) Included on Final Federal 941 Return |
|
||||||||||
|
|
|
|
|
|
|
|
|
||||
Name and Location of Holder of Seller’s Books and Records |
|
|
|
|
|
|
|
|
||||
Certiication: I declare under penalty of perjury that I am the owner, oficer or, member of the business on which tax clearance is requested and that the information is true (Submit a Limited Power of Attorney (Form 3840) if not the owner, oficer, or member).
Print Name |
Title |
|
|
Signature |
|
A business requesting a Michigan Conditional Tax Clearance should forward all uniled Michigan tax returns (up to the date of discontinuance) together with all remittances for those returns with this form to the address below. Mail form directly to: Tax Clearance
Section, Michigan Department of Treasury, P.O. Box 30168, Lansing, MI 48909.
Document Specs
| Fact Name | Details |
|---|---|
| Governing Laws | This form is issued under the provisions of several laws, including Public Act 144 of 1921, Public Act 265 of 1947, Public Act 281 of 1967, Public Act 119 of 1980, Public Act 167 of 1933, and Public Act 94 of 1937. |
| Purpose | The Michigan 514 form is a request for Conditional Tax Clearance for entities that have sold most of their assets but will remain active for tax filing purposes. |
| Eligible Entities | Eligible applicants include sole proprietorships, partnerships, limited liability companies, and corporations. |
| Completion Requirement | The form must be completed in its entirety to ensure processing. Incomplete forms may result in delays. |
| Continuing Business Activity | Applicants must indicate whether they will continue business activity after clearance and provide expected gross receipts for the year if applicable. |
| Escrow Information | If applicable, the form requires information about any money held in escrow pending the receipt of tax clearance. |
| Submission Instructions | The completed form, along with any unfiled Michigan tax returns and remittances, should be mailed to the Tax Clearance Section at the Michigan Department of Treasury. |
Fill out Common Templates
Michigan Des 025 - By adhering to the DES-025 form’s directions, applicants demonstrate compliance with state mandates for their professions.
For landlords seeking to initiate the eviction process, it's vital to utilize the correct documentation to ensure compliance with legal standards. The Illinois PDF Forms provides the necessary resources to fill out the Notice to Quit form accurately, helping to facilitate a smooth transition for both landlords and tenants.
Judgement of Divorce Form Michigan - The formal legal method by which an individual petitioners for divorce in Michigan, stating the irreparable breakdown of the marriage and how ancillary issues are proposed to be settled.