Free Michigan Dch 3877 Template in PDF
The Michigan DCH 3877 form is a critical document utilized in the assessment of individuals who may require mental health services as they transition into nursing facilities. This form, part of the Preadmission Screening and Annual Resident Review (PASARR) process, helps identify potential mental illnesses or developmental disabilities among prospective residents. The DCH 3877 has undergone revisions to better align with current standards and terminologies, including updates to diagnostic references and the renaming of certain service programs. Specifically, it incorporates changes from the Diagnostic and Statistical Manual of Mental Disorders, now using the fourth edition, and modifies terminology from "exception" to "exemption." The form must be filled out by qualified healthcare professionals and includes specific screening criteria that determine whether a comprehensive Level II screening is necessary. Additionally, the DCH 3877 is accompanied by the DCH 3878 form, which certifies exemption criteria in certain cases. Providers can obtain these forms from the Michigan Department of Community Health or download them from the state’s official website. Understanding the DCH 3877 form is essential for healthcare providers involved in the admission and care of individuals in nursing facilities, as it plays a pivotal role in ensuring that residents receive appropriate mental health evaluations and services.
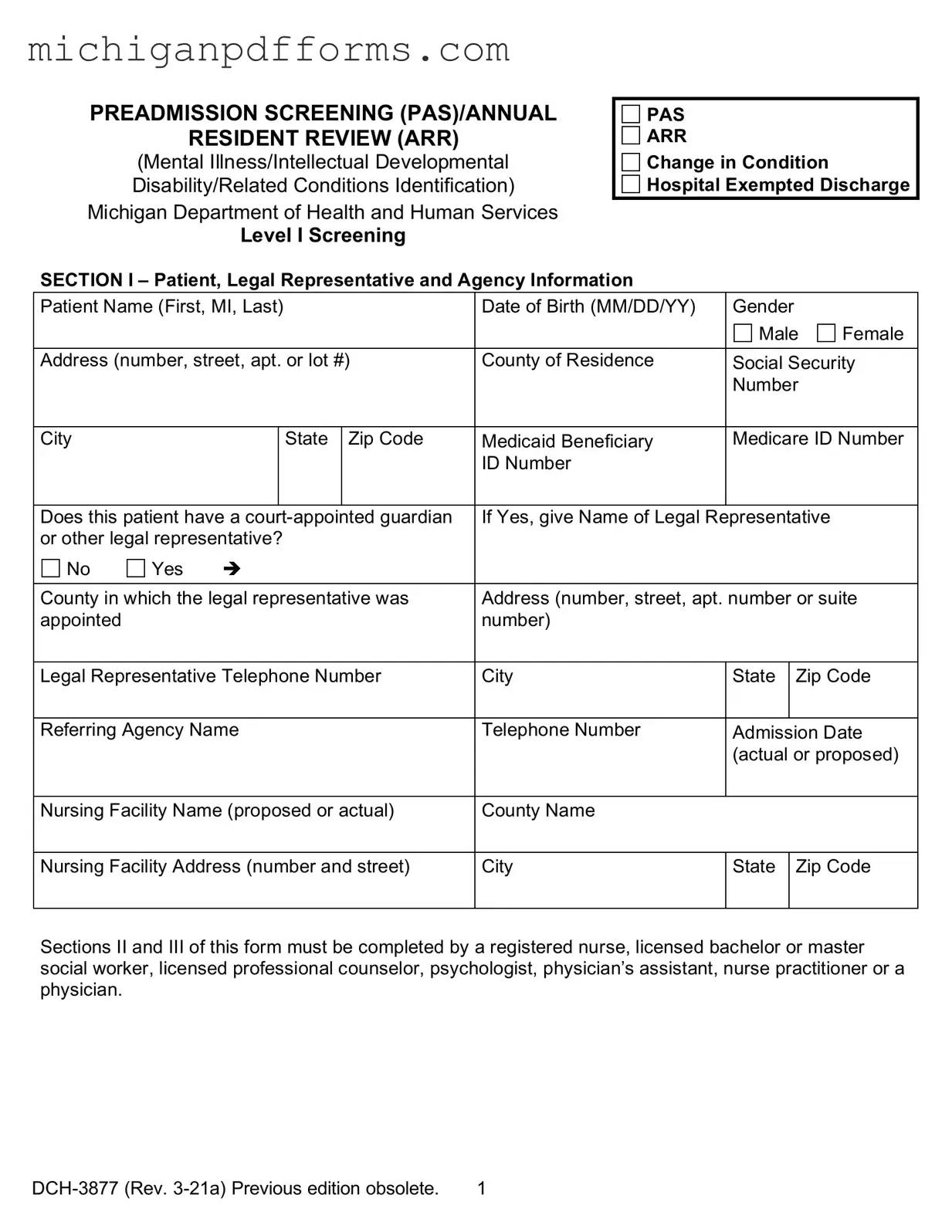
Form Example
PREADMISSION SCREENING (PAS)/ANNUAL
RESIDENT REVIEW (ARR)
(Mental Illness/Intellectual Developmental
Disability/Related Conditions Identification)
Michigan Department of Health and Human Services
Level I Screening
PAS
ARR
Change in Condition
Hospital Exempted Discharge
SECTION I – Patient, Legal Representative and Agency Information
Patient Name (First, MI, Last) |
Date of Birth (MM/DD/YY) |
Gender |
|
|
|||||
|
|
|
|
|
|
Male |
Female |
||
|
|
|
|
|
|
||||
Address (number, street, apt. or lot #) |
County of Residence |
Social Security |
|||||||
|
|
|
|
|
|
Number |
|
||
|
|
|
|
|
|
|
|
||
City |
|
|
State |
Zip Code |
Medicaid Beneficiary |
Medicare ID Number |
|||
|
|
|
|
|
ID Number |
|
|
|
|
|
|
|
|
|
|
|
|||
Does this patient have a |
If Yes, give Name of Legal Representative |
|
|||||||
or other legal representative? |
|
|
|
|
|
||||
No |
Yes |
|
|
|
|
|
|
||
|
|
|
|||||||
County in which the legal representative was |
Address (number, street, apt. number or suite |
||||||||
appointed |
|
|
|
|
number) |
|
|
|
|
|
|
|
|
|
|||||
Legal Representative Telephone Number |
City |
State |
|
Zip Code |
|||||
|
|
|
|
||||||
Referring Agency Name |
Telephone Number |
Admission Date |
|||||||
|
|
|
|
|
|
(actual or proposed) |
|||
|
|
|
|
|
|
||||
Nursing Facility Name (proposed or actual) |
County Name |
|
|
|
|
||||
|
|
|
|
||||||
Nursing Facility Address (number and street) |
City |
State |
|
Zip Code |
|||||
|
|
|
|
|
|
|
|
|
|
Sections II and III of this form must be completed by a registered nurse, licensed bachelor or master social worker, licensed professional counselor, psychologist, physician’s assistant, nurse practitioner or a physician.
1 |
Patient Name |
Date of Birth (MM/DD/YY) |
|
|
|
|
|
|
|
|
SECTION II – Screening Criteria (All 6 items must be completed.) |
|
|
||
1. |
The person has a current diagnosis of Mental Illness or Dementia (Circle one or |
No |
Yes |
|
|
both) |
|
|
|
2. |
The person has received treatment for Mental Illness or Dementia (within the past |
No |
Yes |
|
|
24 months) (Circle one or both) |
|
|
|
3. |
The person has routinely received one or more prescribed antipsychotic or |
No |
Yes |
|
|
antidepressant medications within the last 14 days. |
|
|
|
4. |
There is presenting evidence of mental illness or dementia, including significant |
No |
Yes |
|
|
disturbances in thought, conduct, emotions, or judgment. Presenting evidence may |
|
|
|
|
include, but is not limited to, suicidal ideations, hallucinations, delusions, serious |
|
|
|
|
difficulty completing tasks, or serious difficulty interacting with others. |
|
|
|
5. |
The person has a diagnosis of an intellectual/developmental disability or a related |
No |
Yes |
|
|
condition including, but not limited to, epilepsy, autism, or cerebral palsy and this |
|
|
|
|
diagnosis manifested before the age of 22. |
|
|
|
6. |
There is presenting evidence of deficits in intellectual functioning or adaptive |
No |
Yes |
|
|
behavior which suggests that the person may have an intellectual/developmental |
|
|
|
|
disability or a related condition. These deficits appear to have manifested before the |
|
|
|
|
age of 22. |
|
|
|
Note: If you check “Yes” to items 1 and/or 2, circle the word “Mental Illness” and/or “Dementia.”
Explain any “Yes”
Note: The person screened shall be determined to require a comprehensive Level II OBRA evaluation if any of the above items are "Yes" UNLESS a physician, nurse practitioner or physician’s assistant certifies on form
SECTION III – CLINICIAN’S STATEMENT: I certify to the best of my knowledge that the above information is accurate.
Clinician Signature |
Date |
Name (type or print) |
|
|
|
Address (number, street, apt. number or suite |
Degree/License |
|
number) |
|
|
City
State
Zip Code
Telephone Number
The Michigan Department of Health and Human Services will not exclude from participation in, deny benefits of, or discriminate against any individual or group because of race, sex, religion, age, national origin, color, height, weight, marital status, gender identification or expression, sexual orientation, partisan considerations, or a disability or genetic information that is unrelated to the person’s eligibility.
AUTHORITY: Title XIX of the Social Security Act
COMPLETION: Is voluntary, however, if NOT completed, Medicaid will not reimburse the nursing facility.
DISTRIBUTION: If any answer to items 1 – 6 in SECTION II is "Yes", send ONE copy to the local Community Mental Health Services Program (CMHSP), with a copy of form
2 |
PREADMISSION SCREENING (PAS)/ANNUAL RESIDENT REVIEW (ARR)
Mental Illness/Intellectual Developmental Disability/Related Conditions Identification
Instructions for Completing Level I Screening
This form is used to identify prospective and current nursing facility residents who meet the criteria for possible mental illness or intellectual/developmental disability, or a related condition and who may be in need of mental health services.
Sections II and III must be completed by a registered nurse, licensed bachelor or master social worker, licensed professional counselor, psychologist, physician’s assistant, nurse practitioner or physician.
Preadmission Screening or Hospital Exempted Discharge: The referral source completing the Level I Screening
Annual Resident Review or Change in Condition: This form must be completed by the nursing facility.
Check the appropriate box in the upper
Section II – Screening Criteria – All 6 items in this section must be completed. The following provides additional explanation of the items.
1.Mental Illness: A current primary diagnosis of a mental disorder as defined in the American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders.
Current Diagnosis means that a clinician has established a diagnosis of a mental disorder within the past 24 months. Do NOT mark “Yes” for an individual cited as having a diagnosis "by history" only.
2.Receipt of treatment for mental illness or dementia within the past 24 months means any of the following: inpatient psychiatric hospitalization; outpatient services such as psychotherapy, day program, or mental health case management; or referral for psychiatric consultation, evaluation, or prescription of psychopharmacological medications.
3.Antidepressant and antipsychotic medications mean any currently prescribed medication classified as an antidepressant or antipsychotic, plus Lithium Carbonate and Lithium Citrate.
4.Presenting evidence means the individual currently manifests symptoms of mental illness or dementia, which suggests the need for further evaluation to establish causal factors, diagnosis and treatment recommendations. Further evaluation may need to be completed if evidence of suicidal ideation, hallucinations, delusion, serious difficulty completing tasks or serious difficulty interacting with others.
5.Intellectual/Developmental Disability/Related Condition: An individual is considered to have a severe, chronic disability that meets ALL 4 of the following conditions:
a.It is manifested before the person reaches age 22.
b.It is likely to continue indefinitely.
c.It results in substantial functional limitations in 3 or more of the following areas of major life activity:
3 |
d.It is attributable to:
•Intellectual/Developmental Disability such that the person has significant subaverage general intellectual functioning existing concurrently with deficits in adaptive behavior and manifested during the developmental period;
•cerebral palsy, epilepsy, autism; or
•any condition other than mental illness found to be closely related to Intellectual/ Developmental Disability because this condition results in impairment in general intellectual functioning OR adaptive behavior similar to that of persons with Intellectual/Developmental Disability and requires treatment or services similar to those required for these persons.
6.Presenting evidence means the individual manifests deficits in intellectual functioning or adaptive behavior, which suggests the need for further evaluation to determine the presence of a developmental disability, causal factors, and treatment recommendations. These deficits appear to have manifested before the age of 22.
Note: When there are one or more "Yes" answers to items 1 – 6 under SECTION II, complete form
4 |
Document Specs
| Fact Name | Details |
|---|---|
| Form Purpose | The DCH-3877 is used to identify individuals in nursing facilities who may have mental illness or developmental disabilities. |
| Governing Law | The form is governed by P.A. 280 of 1939 and Title XIX of the Social Security Act. |
| Who Completes It | A registered nurse, social worker, psychologist, physician’s assistant, or physician must complete the form. |
| Distribution | Providers can order the DCH-3877 from the Michigan Department of Community Health or download it from their website. |
| Updates | The DCH-3877 was revised in July 2003 to reflect changes in terminology and diagnostic criteria. |
| Retention Requirement | Nursing facilities must retain the bulletin until the Nursing Facility Manual is updated with the new forms. |
Fill out Common Templates
Immunization Records Michigan - To request a vaccine record, you must fill out the recipient's full name, including any maiden name, and provide the exact date of birth.
Utilizing a complete Medical Power of Attorney guide can empower you to make informed decisions regarding your healthcare directives, ensuring that your wishes are respected even when you cannot voice them. It's crucial to understand the implications of the document and how it functions in varying circumstances.
File a Motion to Set Aside Judgement - Plaintiff and defendant information sections ensure clear identification of all parties involved in the case.