Free Michigan Wc 100 Template in PDF
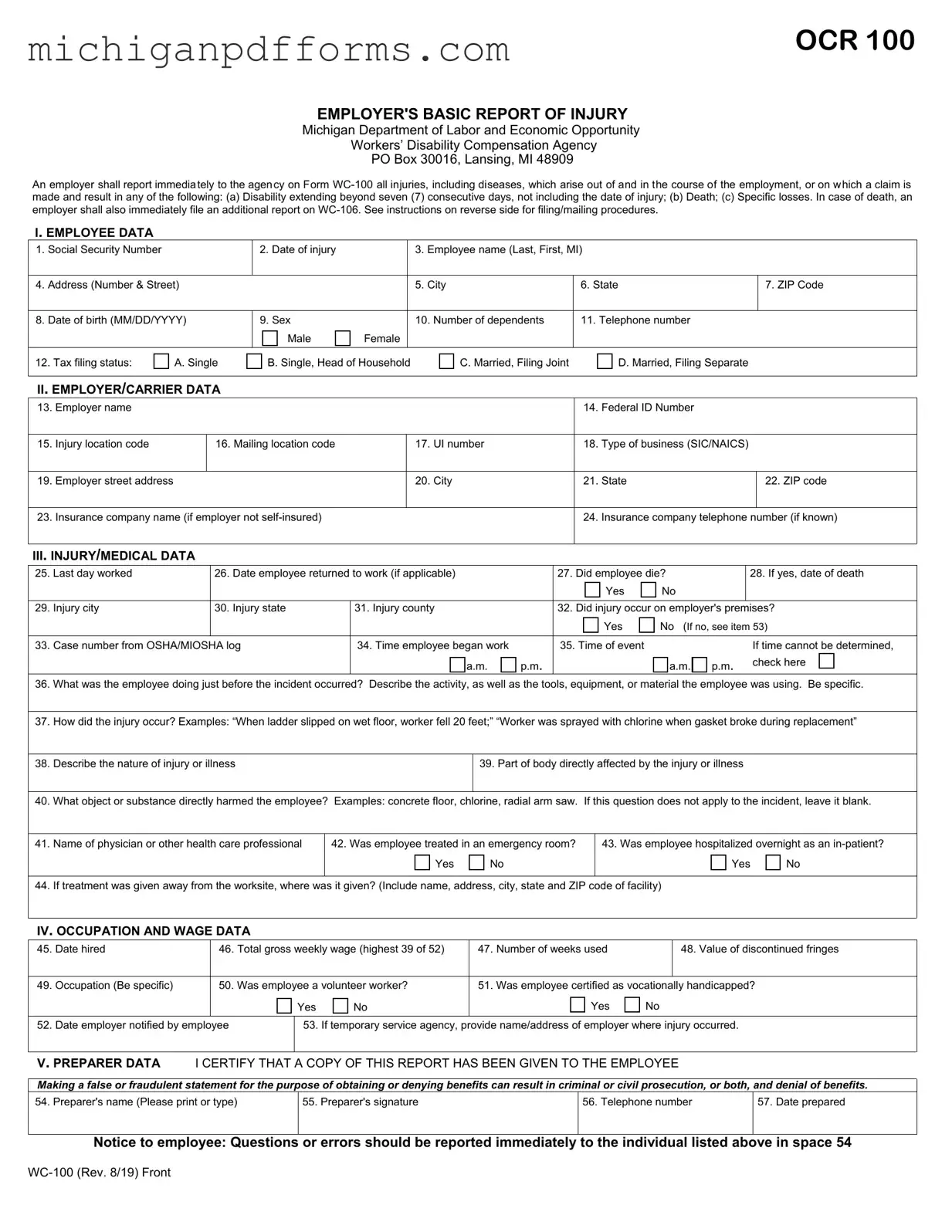
The Michigan WC-100 form serves as a critical document for employers in reporting workplace injuries and illnesses. This form is required to be submitted to the Workers’ Disability Compensation Agency when an employee experiences an injury or disease that arises out of their employment. It is particularly important when the injury results in a disability that lasts beyond seven consecutive days, leads to the death of an employee, or involves specific losses. The WC-100 form collects essential information about the employee, including their personal details, the circumstances surrounding the injury, and any medical treatment received. Employers must provide data regarding their business and the nature of the injury, ensuring compliance with both state and federal regulations. Timely and accurate completion of this form not only fulfills legal obligations but also aids in the management of workers' compensation claims. By adhering to the guidelines outlined in the form, employers can help ensure that affected employees receive the benefits and support they need during their recovery process.
Form Example
OCR 100
EMPLOYER'S BASIC REPORT OF INJURY
Michigan Department of Labor and Economic Opportunity
Workers’ Disability Compensation Agency
PO Box 30016, Lansing, MI 48909
An employer shall report immediately to the agency on Form
I. EMPLOYEE DATA
1. Social Security Number
2. Date of injury
3. Employee name (Last, First, MI)
4. Address (Number & Street)
5. City
6. State
7. ZIP Code
8. Date of birth (MM/DD/YYYY)
12. Tax filing status: |
|
A. Single |
|
9. Sex |
|
|
|
10. Number of dependents |
11. Telephone number |
||||||
|
|
|
Male |
|
Female |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
B. Single, Head of Household |
|
|
C. Married, Filing Joint |
|
|
D. Married, Filing Separate |
||||
|
|
|
|
|
|
|||||||
II. EMPLOYER/CARRIER DATA
13. Employer name
14. Federal ID Number
15. Injury location code
16. Mailing location code
17. UI number
18. Type of business (SIC/NAICS)
19. Employer street address
20. City
21. State
22. ZIP code
23. Insurance company name (if employer not
24. Insurance company telephone number (if known)
III. INJURY/MEDICAL DATA
25. |
Last day worked |
26. Date employee returned to work (if applicable) |
|
27. Did employee die? |
|
|
28. If yes, date of death |
||||||||||||
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
29. |
Injury city |
30. Injury state |
31. Injury county |
|
32. Did injury occur on employer's premises? |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
Yes |
|
No (If no, see item 53) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
33. Case number from OSHA/MIOSHA log |
34. Time employee began work |
|
35. Time of event |
|
|
|
|
If time cannot be determined, |
|||||||||||
|
|
|
|
|
a.m. |
|
p.m. |
|
|
|
|
|
|
a.m. |
|
p.m. |
check here |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
36.What was the employee doing just before the incident occurred? Describe the activity, as well as the tools, equipment, or material the employee was using. Be specific.
37.How did the injury occur? Examples: “When ladder slipped on wet floor, worker fell 20 feet;” “Worker was sprayed with chlorine when gasket broke during replacement”
38. Describe the nature of injury or illness
39. Part of body directly affected by the injury or illness
40. What object or substance directly harmed the employee? Examples: concrete floor, chlorine, radial arm saw. If this question does not apply to the incident, leave it blank.
|
|
|
|
|
41. Name of physician or other health care professional |
42. Was employee treated in an emergency room? |
43. Was employee hospitalized overnight as an |
||
|
Yes |
No |
Yes |
No |
|
|
|
|
|
44. If treatment was given away from the worksite, where was it given? (Include name, address, city, state and ZIP code of facility) |
|
|||
IV. OCCUPATION AND WAGE DATA
45. Date hired
46. Total gross weekly wage (highest 39 of 52)
47. Number of weeks used
48. Value of discontinued fringes
|
|
|
|
|
|
|
|
|
|
|
|
49. Occupation (Be specific) |
50. Was employee a volunteer worker? |
51. Was employee certified as vocationally handicapped? |
|||||||||
|
|
|
Yes |
|
No |
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
||||||
52. Date employer notified by employee |
|
53. If temporary service agency, provide name/address of employer where injury occurred. |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
V. PREPARER DATA I CERTIFY THAT A COPY OF THIS REPORT HAS BEEN GIVEN TO THE EMPLOYEE
Making a false or fraudulent statement for the purpose of obtaining or denying benefits can result in criminal or civil prosecution, or both, and denial of benefits.
54. Preparer's name (Please print or type) |
55. Preparer's signature |
56. Telephone number |
57. Date prepared |
Notice to employee: Questions or errors should be reported immediately to the individual listed above in space 54
If you are using this form as a replacement for the Form 301 to document the specifics of an injury or illness for purposes of compliance with the
If you are using this form to report a workers’ compensation injury, follow the instructions in Section A and B.
Section A
This form can be used in lieu of the MIOSHA Form 301, Injury and Illness Incident Report. It is one of the first f orms you must fill out when a recordable
Within 7 calendar days after you receive information that a recordable
According to Public Law of 1970 (P.L.
form on file for 5 years following the year to which it pertains. DO NOT mail this form to the Workers’ Disability Compensation Agency unless it meets the conditions listed below in Section
B.
Section B
You must complete all questions on this form if the injury or disease results in any of the following: (a) Disability extending beyond seven (7) consecutive days, not including the date of injury; (b) Death; (c) Specific loss. The original form must be mailed to the Workers’ Disability Compensation Agency, P.O. Box 30016, Lansing, MI 48909.
Authority: |
Workers' Disability Compensation Act, 408.31(1)(3) |
Completion: |
Mandatory |
Penalty: |
Workers' Disability Compensation Act, 418.631 |
LEO is an equal opportunity employer/program. Auxiliary aids, services and other reasonable accommodations are available upon request to individuals with disabilities.
Document Specs
| Fact Name | Description |
|---|---|
| Form Purpose | The Michigan WC-100 form is used by employers to report workplace injuries and diseases that arise during employment. |
| Reporting Requirements | Employers must report injuries immediately if they result in disability beyond seven consecutive days, death, or specific losses. |
| Employee Information | The form requires detailed employee data, including Social Security Number, date of birth, and contact information. |
| Employer Information | Employers must provide their name, Federal ID Number, and details about the business and insurance coverage. |
| Injury Details | Specific questions regarding the nature of the injury, treatment, and circumstances surrounding the incident must be answered. |
| Filing Timeline | The form must be completed within seven calendar days of learning about a recordable work-related injury or illness. |
| Governing Law | This form is governed by the Workers' Disability Compensation Act, specifically sections 408.31(1)(3) and 418.631. |
Fill out Common Templates
Transfer of Deed Document - Completing the form involves detailing the specifics of the property transfer, including both the seller’s and buyer’s information.
The Maryland Articles of Incorporation form serves as the foundation for establishing a new corporation within the state. This crucial document outlines the company's basic structure, including its name, purpose, and the details of its incorporators and initial directors. To set your business on the right legal footing, consider filling out the Articles of Incorporation form by clicking the button below.
Loi for Commercial Real Estate Purchase - Specifies conditions related to property inspections and acknowledges agreements made based on inspection findings.